
Key Messages

These are the main health messages that should be conveyed to all future and new parents. They have been written in second person and at a reading level appropriate for the general public so that they can be shared with them directly. They are based on a consensus founded in scientific research and professional practice. Clicking an underlined word or group of words in the text will redirect you to the section in Supporting Evidence section that deals with that topic.
Physical activity has many physical and mental health benefits during pregnancy.
Physical activity during pregnancy can lead to:
- Less stress.
- More energy.
- More oxygen for your baby.
- Better posture.
- A healthy weight gain.
- Less risk of developing pregnancy-related diabetes or high blood pressure.
- An easier recovery after birth.
Speak to your health care provider before changing or beginning an exercise routine.
If you do not have medical conditions that prevent you from exercising during pregnancy and if you are already physically active (i.e., you exercise for 150 minutes per week at moderate or vigorous intensity), you can continue to accumulate at least 150 minutes of moderate-intensity physical activity each week over a minimum of three days per week. Being active every day is encouraged. Include a variety of aerobic and resistance training activities to achieve greater benefits. Adding yoga or gentle stretching may also be beneficial.
Moderate-intensity exercise raises your heart rate and leaves you slightly out of breath. If you are unable to talk and carry on a conversation during exercise, is it too intense.
If you do not already exercise but would like to, it is best to gradually work up to at least 150 minutes of moderate-intensity exercise over a minimum of three days per week.
You don’t have to go to the gym to be active. Physical activity can easily be added to your daily routine.
Being active is a fun way to meet new people and is a great way to spend time with your partner or friends. It can set the stage for active family living.
Some physical activities you may enjoy during pregnancy include:
- Walking.
- Jogging.
- Swimming.
- Dancing.
- Stationary bicycling.
- Housework.
You may also enjoy wellness activities such as meditation, visualization, and deep breathing. They can reduce your stress level and be useful during labour and birth to decrease the intensity of pain.
Not all activities are safe during pregnancy. High-intensity activities, heavy lifting, and activities which could cause you to fall or injure yourself should be avoided.
Physical activities which you should avoid during pregnancy include:
- Horseback riding.
- Downhill skiing.
- Hockey.
- Gymnastics.
- Mountain biking.
- Scuba diving.
After your fourth month (16 weeks) of pregnancy, change any exercises that you would normally do on your back. You may be able to do them on your side, or while you are standing or sitting. Lying on your back can decrease the amount of blood flow to your baby.
When you are exercising, listen to your body and know when to stop.
Being active takes slightly more effort during pregnancy. You may tire a bit faster than before. Your baby is growing, and this takes energy. Your body is also changing, which affects what you can do. You should not go over a specific heart rate zone which corresponds to your age, current activity level, and weight. Pregnancy is also not the time to train for an athletic competition.
During exercise, drink plenty of water and try not to get too hot. Avoid hot yoga, the use of hot tubs and saunas, and prolonged time periods outside in the sun.
Pelvic floor exercises, during pregnancy and after birth, can help reduce the risk of urinary incontinence.
Some women will experience urinary leakage during pregnancy or after birth. This can occur due to weakened pelvic floor muscles (the muscles between your anus and vagina).
You can do simple, daily pelvic floor exercises, such as Kegel exercises, throughout your pregnancy to strengthen your pelvic floor muscles. Ask your health care provider how to do Kegel exercises effectively.
Learn more about exercise in pregnancy.
You can find out more about exercise in pregnancy from the following resources. More suggestions can be found in the Resources and Links section.
- Your health care provider
- Your local public health unit 1-866-532-3161
- oMama
Supporting Evidence
About Physical Activity during Pregnancy
For years, it was believed that women should reduce their level of physical activity during pregnancy, and that pregnancy was a time to effectively ‘put one’s feet up’. Current research debunks such thinking.1,2 It is now widely established that pregnant women who do not have any extenuating medical conditions should participate in regular, moderate-intensity physical activity after consultation with their health care provider in order to gain optimal health benefits for themselves and their developing offspring.1,2,3,4,5,6
It is reported that many more women today want to maintain their current fitness level during pregnancy and that others want to initiate an exercise program during pregnancy due to its many benefits.2 Despite this information, women in Ontario7and elsewhere8,9 are still not meeting the recommended guidelines for physical activity during pregnancy.
The Canadian Community Health Survey (2005 – 2008) found that among 623 pregnant women aged 15 – 49 years in Ontario only 58 percent participated in regular physical activity (15 minutes or more on at least three days of the week), and only 23 percent met the Canadian guidelines for physical activity during pregnancy (30 minutes on four days per week). It was also found that women were less likely to meet the national guidelines for physical activity during pregnancy if they were single, divorced, separated, or widowed; a visible minority; or had a household income between $20,000 and $79,999.7
Many pregnant women want to engage in aerobic exercise during pregnancy, but still seem to be concerned about possible, adverse effects on their pregnancy outcome.7,8,9,10 Promoting physical activity and its benefits during pregnancy, needs to become a stronger health education message.7,11 Women need to be given information on the benefits of physical activity during pregnancy, and be given the opportunity to discuss their concerns about physical activity during pregnancy. They can be encouraged to develop a safe exercise routine, which they are comfortable engaging in throughout their pregnancy.7,11
Women often feel that they need a social support system as well as economic resources to achieve their exercise goals during pregnancy. Women can be encouraged to incorporate physical activity into their daily life. This can include household chores, walking, dancing, or participating in sports. Many communities have walking groups and pregnancy fitness classes. This information may be especially beneficial for those who do not have a strong social support system. The social determinants of health cannot be forgotten when educating pregnant women on the importance of physical activity during pregnancy.7,12
Benefits of Physical Activity during Pregnancy
The benefits associated with physical activity are numerous. Some of the benefits associated with physical activity during pregnancy for women include:5,6,7,8,12,13,14,15,16,17,18
- Increased cardiovascular function (improving maternal-placental blood flow).
- Decreased risk of excessive gestational weight gain.
- Decreased musculoskeletal pain (especially lower-back pain).
- Decreased muscle cramps.
- Decreased lower-limb edema.
- Decreased risk of developing varicose veins and deep vein thrombosis.
- Decreased risk of developing gestational diabetes.
- Decreased risk of developing hypertension and pre-eclampsia.
- Decreased symptoms of anxiety and depression.
- Decreased fatigue.
- Improved coping skills.
- Increased self-confidence.
- Decreased length of labour (in some cases).
- Decreased need for instrument-assisted birth.
Some of the benefits associated with physical activity during pregnancy for a developing fetus include:3,13,18,19
- Decreased risk of preterm delivery.
- Increased heart rate variability of the fetus.
- Decreased risk of a low birth-weight infant.
- Decreased risk of childhood obesity.
Recommended Activities during Pregnancy
Canadian recommendations for physical activity during pregnancy for women with no adverse risks include at least 150 minutes of moderate-intensity physical activity each week over a minimum of three days per week. Being active every day is encouraged. Include a variety of aerobic and resistance training activities to achieve greater benefits. Adding yoga or gentle stretching may also be beneficial 78.
Aerobic exercise of moderate-intensity requires a woman to increase her heart rate and breathing pattern and to lightly perspire. Its purpose is to effectively stimulate the cardiovascular and the cardiorespiratory systems of the body.20
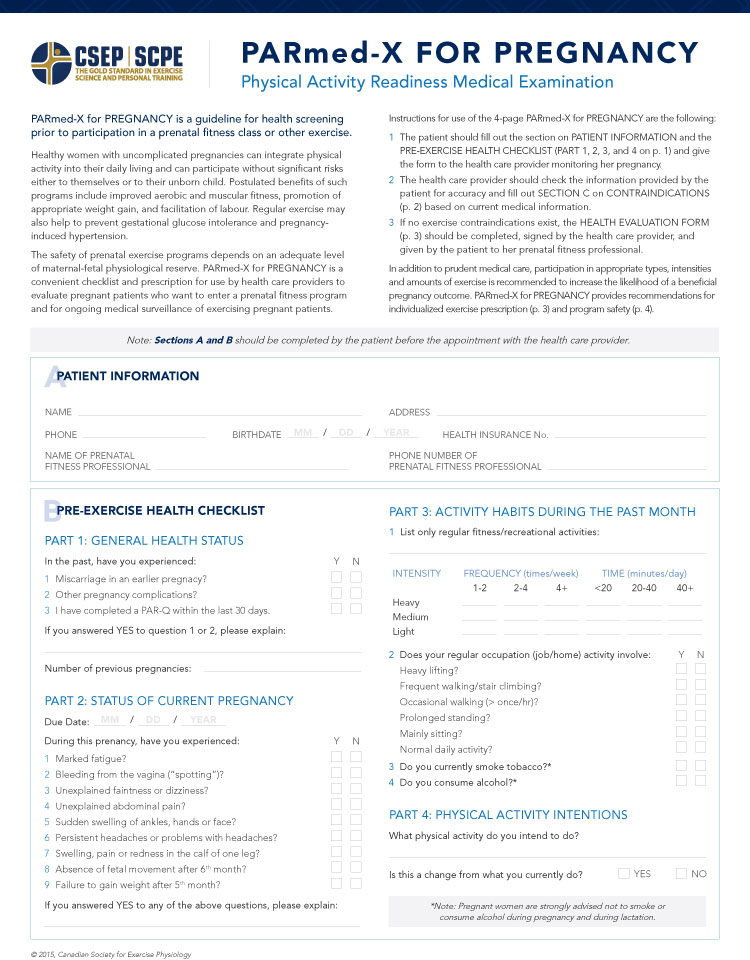
If women are already physically active and have no risks associated with physical activity during pregnancy, they will likely be able to continue a similar exercise regimen during pregnancy. Pregnant women are advised to consult with their health care provider to clarify risks and make modifications to any physical activities. The Physical Activity Readiness Medical Examination for Pregnancy ( PARmed-X for pregnancy) can be used as part of this process.4,6
While women should be encouraged to be active during pregnancy and to participate in activities that they enjoy, pregnancy is not the time to try to reach optimum fitness goals or to train for strenuous fitness competitions.2,4,18
Initiating an aerobic exercise program during pregnancy
It is recommended that sedentary women who want to begin to exercise during their pregnancy gradually increase the amount of exercise that they engage in.
They should begin with 15-minute sessions three days a week and gradually increase to at least 150 minutes of moderate-intensity exercise over a minimum of three days per week, at the appropriate target heart rate for them. It is important for women to listen to their bodies and reduce or increase activity when they feel ready.4,6, 78
The following is a list of aerobic activities recommended during pregnancy:4,21,22
- Brisk walking.
- Cycling indoors on a stationary bike.
- Dancing.
- Swimming.
- Water aerobics.
- Low-impact aerobics.
- Cross-country skiing (with care taken not to fall).
- Snowshoeing (with care taken not to fall).
- Exercising on a stair trainer, elliptical machine, or other cardio machines in a fitness centre or at home.
These activities are recommended during pregnancy as they pose a reduced risk for women to lose their balance or fall . They activities also cause minimal trauma to joints and ligaments.21,22
Water aerobics
Exercising in aquatic environments is highly recommended during pregnancy.1,23,24,25
It has been shown to decrease joint stress, lower-back pain, and edema in the lower extremities. It can also improve mobility, increase blood flow, and increase overall comfort levels for pregnant women as the buoyancy of the water helps support the enlarging uterus.1,25
Water aerobics (or aqua-fit) can be especially beneficial in the third trimester of pregnancy when the size of a woman’s abdomen, perception of clumsiness, and lower-back pain tend to be the greatest.1
Nurturing the mind and supporting positive mental health during pregnancy is as important as physical activity. During pregnancy, women can be exposed to a variety of psychological stressors. If women do not adequately address these stressors, biological responses can be triggered that can lead to detrimental health outcomes.18
Wellness activities include yoga, tai chi, meditation, visualization, and deep breathing. They involve a variety of benefits and are available for a low cost, if any, and can be performed daily.26
Yoga
Yoga is an ancient Indian tradition that combines physical and spiritual practices. It is becoming increasingly popular as it confers many physical and physiological benefits.27
Yoga involves three elements simultaneously:27
- Asana (postures).
- Pranayama (breathing techniques).
- Dhyana (meditation).
The benefits of yoga during pregnancy include:26,28,29,30,31,32,33
- Improved muscular strength.
- Improved cardiovascular fitness.
- Lower blood pressure.
- Improved immune functioning.
- Less aches and pain.
- Improved mood.
- Improved ability to sleep.
- Reduction in the risk of preterm labour.
- Shorter length of labour.
Prenatal yoga classes, specifically for pregnant women, are available in many major urban centres across Canada. Certain yoga poses are less appropriate during pregnancy, and variations can be provided.29,33
Tai chi
Tai chi is a Chinese martial art that involves slow, steady movements. It can improve balance and decrease symptoms of anxiety, depression, and insomnia among pregnant women.26,34
Meditation
Meditation, or mindfulness, is traditionally a Buddhist practice which involves forming an astute sense of mental awareness and openly accepting one’s current thoughts, sensations, bodily states, and environment. Its purpose is to promote self-reflection and to practice managing difficult emotions.35,36,37
Meditation generally requires:38
- A quiet place.
- A comfortable position (seated, standing, walking, side-lying).
- Focused attention on a mantra, an object, or the sensation of breathing.
- An open mind towards distracting thoughts that may arise.
Women who practice meditation during pregnancy can experience decreased levels of anxiety and stress.37,39,40
Visualization
Visualization, or guided imagery, helps people cope with challenges they face in life by imagining positive outcomes.41,42
Assisting a woman to look forward to her life with her baby, for example, can help her cope with some of the challenges in her pregnancy. If a woman is unable to visualize positive outcomes on her own, CDs with positive affirmations are available.42
Deep breathing
Deep breathing exercises require a person be calm, focused, and engaged in a rhythmic pattern of breathing in and breathing out. Women who engage in such exercises during pregnancy can increase their level of relaxation, improve their oxygen saturation, and decrease their perception of pain through distraction. 43
Deep breathing exercises combined with light aerobic exercises, like bouncing on a birthing ball, can provide increased distraction from pain.22
Deep breathing can be useful during labour. It is best to practice deep breathing during pregnancy to optimize these benefits during labour.43 See the Labour Support file for more information on breathing techniques.
Precautions
Women need to be mindful of the intensity level while engaging in aerobic exercise during pregnancy. Exercise that is too intense may compromise fetal well-being by restricting utero-placental blood flow.44,45 The intensity of aerobic exercise can be evaluated using the talk test and target heart rate zones.4,6
The talk test
The talk test is a simple way to evaluate the intensity of physical activity. During moderate-intensity aerobic exercise, a pregnant woman should feel slightly out of breath but should still be able to carry on a conversation. If she cannot, she should reduce the intensity of her workout.4,6
Target heart rate zones
A more objective way to monitor the intensity level of exercise during pregnancy is through heart rate monitoring.4,6,46
During pregnancy, a woman’s resting heart rate increases by approximately 10 – 15 beats per minute. This increase in resting heart rate compensates for the increased demands of the growing fetus. As a result, the maximum target heart rate during pregnancy decreases.4,47
An age-corrected heart rate target zone for pregnant women has been developed, which also takes into account a woman’s current activity level and BMI (Table 1).6 It is important that women who are starting a new exercise program or who are at the end of their pregnancy stay in the lower end of their heart rate target zone.4
Pregnancy raises body temperature. This results in an increase in perspiration. If water loss from sweating is greater than fluid intake, dehydration can occur. It is important that women stay well hydrated during pregnancy. Pregnant women should not wait until they are thirsty to drink. It is recommended that pregnant women drink before, during, and after physical activity to avoid dehydration.48,49
The signs of dehydration (from light to moderate effects) are:50
- Poor skin turgor.
- Feeling thirsty.
- Inability to spit.
- Dry mucous membranes.
- Sunken eyes.
A pregnant woman’s increased body temperature increases her risk of heat stroke and hyperthermia.49 Hyperthermia in pregnancy increases the risk of neural tube defects.53,54
During pregnancy, women should avoid practicing Bikram (hot) yoga, sitting in a hot tub, and exercising in very hot weather or humid environments.53,54,55
When exercising indoors, pregnant women should be encouraged to use a cooling fan to prevent overheating.56
While physical activity is highly encouraged, there are some activities that pregnant women should avoid.4,6,56
Dangerous activities
Activities such as horseback riding, downhill skiing, ice hockey, gymnastics, and mountain biking on difficult trails should be avoided during pregnancy. These activities can cause a loss of balance and trauma which can, consequently, put a fetus at risk of harm.4,56 Exercise guidelines for pregnant women do not recommend activities involving risks of falls, trauma, or collisions.57
Activities involving extreme or reduced air pressures
Activities that involve changes in pressure such as scuba diving or hiking or climbing above 1,600 meters should be avoided during pregnancy as a fetus is not protected from the effects of decompression sickness.4,58 If pregnant women do engage in these activities, they should decrease the intensity of the activity they are engaging in.4
Heavy lifting
Heavy lifting can trigger the Valsalva manoeuvre (i.e., holding one’s breath while working against a resistance). This can cause a change in blood pressure, which should be minimized during pregnancy. Heavy lifting can also increase women’s susceptibility to joint injury due to the accumulation of a hormone called relaxin during pregnancy.6,59,60
Women should be advised that if they do heavy lifting or a lot of bending and stooping at their place of employment, they may need to modify their work during pregnancy.60
If strength training is done during pregnancy, women should focus on correct form and use lighter weights.6,59,60 Women should also ensure that they breathe through the activity, exhaling on exertion and inhaling on relaxation.6
Supine position
It is recommended that pregnant women avoid prolonged exercise flat on their back during pregnancy, especially after 16-weeks’ gestation. The enlarged uterus can put pressure on the inferior vena cava (the vein that returns blood from the lower extremities to the heart) and the abdominal aorta (the main blood supply to the uterus).
This pressure can cause dizziness, shortness of breath, and reduced utero-placental circulation, which can affect fetal well-being. To avoid this effect, activities can be modified to be done in side-lying, sitting, or standing position.6,61,62
If a pregnant woman experiences any of the following symptoms (which rarely occur), it is strongly recommended that the activity be stopped and a health care provider be consulted:4,6,56,57
- Dizziness or fainting.
- Blurred vision.
- Excessive shortness of breath.
- Chest pain.
- Abnormally high heart rate that does not drop when the activity is stopped.
- Pain or edema in the calves.
- Sudden swelling of hands, face, or feet.
- Sudden change in body temperature.
- Strong, sharp pain in the pubis, back, abdomen, or chest.
- Painful uterine contractions.
- Vaginal bleeding.
- Any gush of fluid from the vagina.
Urinary Incontinence and Pelvic Floor Exercises
The pelvic floor is comprised of a group of muscles and ligaments, which support the bladder, the uterus, and the bowel. The pelvic floor muscles attach to the pubic bone at the front and the tail bone at the back and run along the base of the pelvis. Due to their location inside the pelvis, the pelvic floor muscles are the only group of muscles in the body which provide structural support for the urethra, the vagina, and the rectum (the organs with openings that pass through the pelvic floor).63
Under normal conditions, a conscious, voluntary contraction of the pelvic floor muscles results in a squeeze and an inward lift causing the urethra to close, stabilize, and resist downward movement.64,65
When the pelvic floor muscles are strong, they support the pelvic organs to prevent problems such as:63,66
- Incontinence (the involuntary loss of urine or faeces).
- Prolapse (or disposition) of the bladder, uterus, and bowel.
Figure 1 shows the difference between normal pelvic floor muscles and weakened pelvic floor muscles and their effect on internal organ positioning.
It is very common for pregnancy and childbirth to cause the pelvic floor muscles to weaken.67,68 It is estimated that about 50 percent of women lose some of the supporting function of the pelvic floor during pregnancy and childbirth.68 The greatest damage to the pelvic floor usually occurs during women’s first vaginal delivery, especially if assisted birth (vacuum or episiotomy) is utilized.67,69
If women have a caesarean birth, the effects of pregnancy can still cause their pelvic floor muscles to weaken.70,71
Weakening of the pelvic floor muscles can cause:63,66,67
- Urinary incontinence.
- Fecal incontinence.
- Pelvic organ prolapse.
- Sensory and emptying abnormalities.
- Sexual dysfunction.
- Chronic pain.
The most common effect is urinary incontinence.70,71 It is estimated that approximately one-third of women suffer from urinary incontinence after birth.71 For women who experience incontinence for more than three months following birth, there is an increased risk that it will persist for more than five years.69
Urinary incontinence can cause reduced quality of life for women. Involuntary urinary leakage can occur during activities such as coughing, laughing, sneezing, or engaging in physical activity.67,71
The pelvic floor muscles are like any other muscles in the body requiring exercise to keep them strong and healthy. Pelvic floor exercises, or pelvic muscle-clenching exercises, strengthen and prevent muscle damage and improve urinary continence. It is critically important to encourage women to engage in pelvic floor exercises during and after pregnancy.63,64,67,69,70,71,72,73,74,75
Kegel exercise
One of the simplest types of pelvic floor exercises is commonly referred to as the Kegel exercise named after Dr. Arnold Kegel who first developed it. A Kegel exercise involves consciously contracting the muscles of the perineum to increase their tone and strength.72
One of the obstacles that decrease women’s motivation to do pelvic floor exercises is insufficient knowledge on how to perform them properly. Teaching women how to properly contract this muscle group encourages women to do the exercises.74 A physiotherapist who specializes in pelvic floor rehabilitation can help with this.
The following is a description on how to do Kegel exercises:72
- Stand, sit, or lie down with your knees slightly apart (lie down if just beginning).
- Relax.
- Imagine that you are trying to hold back urine or a bowel movement. Squeeze the muscles you would use to do that. DO NOT tighten your stomach or buttocks.
- Tighten the muscles for 5 to 10 seconds. Make sure you keep breathing normally.
- Now relax the muscles for about 10 seconds.
- Repeat 12 to 20 times, three to five times a day.
It is important for women to continue to do this exercise throughout their lives. Like any other muscle in the body, pelvic floor muscles only remain strong if they are exercised regularly.72
If women have difficulty focusing on the muscles to contract, they can insert a finger into their vagina to feel the muscle contraction. When contracting, they should feel pressure around their finger and not feel pressure expelling the finger out.71
Women can promote better recovery of their pelvic floor muscles after birth by: 76,77
- Maintaining adequate hydration and a healthy diet. This can prevent constipation, which can cause pelvic floor muscles to weaken further.
- Resuming low-impact exercises such as walking and swimming once given clearance by their health care provider to do so.
- Refraining from participating in high-impact sports such as running and jumping rope, which can increase pressure on the pelvic floor muscles.
- Refraining from strenuous efforts such as lifting the baby in its car seat until sufficient muscle strength has returned.
For exercise suggestions, see the Physical Activity Resource Centre (PARC) Active Pregnancy resource in the Resources and Links section.
The pelvic floor muscles have regained sufficient strength if the following conditions are present:66
- Good control of gas, faeces, and urine.
- The ability to stop urine mid-stream.
Referrals
Women and/or her support people may need to be referred for additional support if they:
- Are overly anxious about exercising during pregnancy.
- Are considering engaging in exercise above the recommended guidelines.
- Need more information about how to maintain or start exercising during pregnancy.
- Need support in doing pelvic floor exercises.
Women and/or her support people who need more information about exercise and active living during pregnancy may be referred to
- Their health care provider (obstetrician, family physician, nurse practitioner, or midwife).
- A physiotherapist who offers specialized pelvic health services.
- An exercise physiologist, or sports medicine specialist.
Resources & Links
Professional Guidelines
- Canadian Academy of Sport and Exercise Medicine (CASEM)
- Canadian Society for Exercise Physiology (CSEP)
- Society of Obstetricians and Gynaecologists of Canada (SOGC)
- Clinical Practice Guideline: Exercise in Pregnancy and the Postpartum Period (2003)
- 2019 Canadian Guideline for Physical Activity throughout Pregnancy (2018)
Professional Associations
Reports/Publications
- Davenport, M. H., Charlesworth, S., Vanderspank, D., Sopper, M. M., & Mottola, M. F. (2008). Development and validation of exercise target heart rate zones for overweight and obese pregnant women. Applied Physiology, Nutrition, and Metabolism, 33(5), 984-989. doi:10.1139/H08-086
- Dumoulin, C., & Hay-Smith, J. (2010). Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database of Systematic Reviews, 1(CD005654), 1-51. doi: 10.1002/14651858.CD005654.pub2
- Mottola, M. F., Davenport, M. H., Brun, C. R., Inglis, S. D., Charlesworth, S., & Sopper, M. M. (2006). VO2peak prediction and exercise prescription for pregnant women. Medicine and Science in Sports and Exercise, 38(8), 1389-1395. doi: 10.1249/01.mss.0000228940.09411.9c
Websites
- Canadian Continence Foundation
- Ontario Physiotherapy Association
- Pelvic Health Solutions
- Public Health Agency of Canada
- The Healthy Pregnancy Guide
- Society of Obstetricians and Gynaecologists of Canada (SOGC)
- Western University
Helplines
- Motherisk
1-877-439-2744 (Toll-free)
416-813-6780 (Toronto and GTA)
Prenatal Education Provider Tools
- Best Start Resource Centre
- Prenatal Education Program: Module 4 - Physical & Emotional Fitness (2017)
Client Resources and Handouts
- Canadian Continence Foundation
- Public Health Agency of Canada
Books
- Nordahl, K., Petersen, C, & Jeffreys, R. (2005). Fit to deliver: An innovative prenatal and postpartum fitness program. Vancouver, BC: Hartley & Marks Publishers Inc.
Videos
- Western University
Apps
Appendix
References
- Charlesworth, S., Foulds, H. J., Burr, J. F., & Bredin, S. S. (2011). Evidence-based risk assessment and recommendations for physical activity clearance: Pregnancy. Applied Physiology, Nutrition, and Metabolism, 36(1), 33-48. doi:10.1139/H11-061
- Downs, D. S., Chasan-Taber, L., Evenson, K. R., Leiferman, J., & Yeo, S. (2012). Physical activity and pregnancy: Past and present evidence and future recommendations. Research Quarterly for Exercise and Sport, 83(4), 485-502. doi:10.1080/02701367.2012.10599138
- Both, M. I., Overvest, M. A., Wildhagen, M. F., Golding, J., & Wildschut, H. I. (2010). The association of daily physical activity and birth outcome: A population-based cohort study. European Journal of Epidemiology, 25(6), 421-429. doi:10.1007/s10654-010-9458-0
- Davies, G. A., Wolfe, L. A., Mottola, M. F., & MacKinnon, C. (2003). Joint SOGC/CSEP clinical practice guideline: Exercise in pregnancy and the postpartum period. Canadian Journal of Applied Physiology, 28(3), 329-341.
- Ferraro, Z. M., Gruslin, A., & Adamo, K. B. (2013). An active pregnancy for fetal well-being? The value of active living for most women and their babies. British Journal of Sports Medicine, 47(13), 813-814. doi:10.1136/bjsports-2012-091452
- Canadian Society for Exercise Physiology. (2013). PARmed-X for pregnancy: Physical activity readiness medical examination. Retrieved from http://www.csep.ca/cmfiles/publications/parq/parmed-xpreg.pdf
- Gaston, A., & Vamos, C. A. (2013). Leisure-time physical activity patterns and correlates among pregnant women in Ontario, Canada. Maternal and Child Health Journal, 17(3), 477-484. doi:10.1007/s10995-012-1021-z
- Borodulin, K., Evenson, K. R., Wen, F., Herring, A. H., & Benson, A. (2008). Physical activity patterns during pregnancy. Medicine & Science in Sports & Exercise, 40(11), 1901-1908. doi:10.1249/MSS.0b013e31817f1957
- Fell, D. B., Joseph, K. S., Armson, B. A., & Dodds, L. (2009). The impact of pregnancy on physical activity level. Maternal and Child Health Journal, 13(5), 597-603. doi:10.1007/s10995-008-0404-7
- Kramer, M. S., & McDonald, S. W. (2006). Aerobic exercise for women during pregnancy. Cochrane Database of System Reviews, 2006(3), 1-57. doi:10.1002/14651858.CD000180.pub2
- Leiferman, J., Swibas, T., Koiness, K., Marshall, J. A., & Dunn, A. L. (2011). My baby, my move: Examination of perceived barriers and motivating factors related to antenatal physical activity. Journal of Midwifery & Women’s Health, 56(1), 33-40. doi: 10.1111/j.1542-2011.2010.00004.x
- Fieril, K. P., Olsén, M. F., Glantz, A., & Larsson, M. (2014). Experiences of exercise during pregnancy among women who perform regular resistance training: A qualitative study. Physical Therapy, 94(8), 1135-1143. doi:10.2522/ptj.20120432
- Melzer, K., Schutz, Y., Boulvain, M., & Kayser, B. (2010). Physical activity and pregnancy. Sports Medicine, 40(6), 493-507. doi:0112-1642/10/0006-0493/$49.95/0
- Hui, A., Back, L., Ludwig, S., Gardiner, P., Sevenhuysen, G., Dean, H., . . . Shen, G. X. (2012). Lifestyle intervention on diet and exercise reduced excessive gestational weight gain in pregnant women under a randomised controlled trial. BJOG: An International Journal of Obstetrics & Gynaecology, 119(1), 70-77. doi:10.1111/j.1471-0528.2011.03184.x
- Ruchat, S. M., Davenport, M. H., Giroux, I., Hillier, M., Batada, A., Sopper, M. M., . . . Mottola, M. F. (2012). Nutrition and exercise reduce excessive weight gain in normal-weight pregnant women. Medicine and Science in Sports and Exercise, 44(8), 1419-1426. doi:10.1249/MSS.0b013e31825365f1
- Streuling, I., Beyerlein, A., & von Kries, R. (2010). Can gestational weight gain be modified by increasing physical activity and diet counseling? A meta-analysis of interventional trials. American Journal of Clinical Nutrition, 92(4), 678-687. doi:10.3945/ajcn.2010.29363
- Wolfe, L. A., & Mottola, M. F. (2000). Validation of guidelines for aerobic exercise in pregnancy. In D. A. Kumbhare & J. V. Basmajian (Eds.), Decision-making and outcomes in sports rehabilitation (pp. 205-222). New York, NY: Churchill Livingstone.
- Beddoe, A. E., & Lee, K. A. (2008). Mind-body interventions during pregnancy. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 37, 165-175. doi:10.1111/j.1552-6909.2008.00218.x
- May, L. E., Scholtz, S. A., Suminski, R., & Gustafson, K. M. (2014). Aerobic exercise during pregnancy influences infant heart rate variability at one month of age. Early Human Development, 90(1), 33-38. doi:10.1016/j.earlhumdev.2013.11.001
- Kramer, M. S., & McDonald, S. W. (2006). Aerobic exercise for women during pregnancy. Cochrane Database of System Reviews, 2006(3), 1-57. doi:10.1002/14651858.CD000180.pub2
- Wolfe, L. A. (2000). Pregnant women and endurance exercise. In R. J. Shephard & P.O. Åstrand (Eds.), Endurance in sport (2nd ed.) (pp. 531-546). London, UK: Blackwell Scientific
- Yan, C. F., Hung, Y. C., Gau, M. L., & Lin, K. C. (2014). Effects of a stability ball exercise programme on low back pain and daily life interference during pregnancy. Midwifery, 30(4), 412-419. doi:10.1016/j.midw.2013.04.011
- Irion, J. M., & Irion, G. L. (2011). Water immersion to reduce peripheral edema in pregnancy. Journal of Women’s Health Physical Therapy, 35(2), 46-49. doi:10.1097/JWH.0b013e318225f18a
- Vallim, A. L., Osis, M. J., Cecatti, J. G., Baciuk, É. P., Silveira, C., & Cavalcante, S. R. (2011). Water exercises and quality of life during pregnancy. Reproductive Health, 8, 1-14. doi:10.1186/1742-4755-8-14
- Waller, B., Lambeck, J., & Daly, D. (2009). Therapeutic aquatic exercise in the treatment of low back pain: A systematic review. Clinical Rehabilitation, 23(1), 3-14. doi:10.1177/0269215508097856
- Field, T., Diego, M., Delgado, J., & Medina, L. (2013). Tai chi/yoga reduces prenatal depression, anxiety and sleep disturbances. Complementary Therapies in Clinical Practice, 19(1), 6-10. doi:10.1016/j.ctcp.2012.10.001
- Chapman, K. L., & Bredin, S. S. (2011). Why Yoga? An introduction to philosophy, practice, and the role of yoga in health promotion and disease prevention. The Health & Fitness Journal of Canada, 3(2), 13-21.
- Chuntharapat, S., Petpichetchian, W., & Hatthakit, U. (2008). Yoga during pregnancy: Effects on maternal comfort, labor pain and birth outcomes. Complementary Therapies in Clinical Practice, 14(2), 105-115. doi:10.1016/j.ctcp.2007.12.007
- Curtis, K., Weinrib, A., & Katz, J. (2012). Systematic review of yoga for pregnant women: Current status and future directions. Evidence-Based Complementary and Alternative Medicine, 2012, 1-13. doi:10.1155/2012/715942
- Maharana, S., Nagarathna, R., Padmalatha, V., Nagendra, H. R., & Hankey, A. (2013). The effect of integrated yoga on labor outcome: A randomized controlled study. International Journal of Childbirth, 3(3), 165-177. http://dx.doi.org/10.1891/2156-5287.3.3.165
- Narendran, S., Nagarathna, R., Narendran, V., Gunasheela, S., & Nagendra, H. R. R. (2005). Efficacy of yoga on pregnancy outcome. Journal of Alternative & Complementary Medicine, 11(2), 237-244. doi:10.1089/acm.2005.11.237
- Satyapriya, M., Nagarathna, R., Padmalatha, V., & Nagendra, H. R. (2013). Effect of integrated yoga on anxiety, depression & well-being in normal pregnancy. Complementary Therapies in Clinical Practice, 19(4), 230-236. doi:10.1016/j.ctcp.2013.06.003
- Field, T. (2011). Yoga clinical research review. Complementary Therapies in Clinical Practice, 17(1), 1-8. doi:10.1016/j.ctcp.2010.09.007
- Dunning, K., LeMasters, G., & Bhattacharya, A. (2010). A major public health issue: The high incidence of falls during pregnancy. Maternal and Child Health Journal, 14(5), 720-725. doi:10.1007/s10995-009-0511-0
- Bishop, S. R. (2002). What do we really know about mindfulness-based stress reduction? Psychosomatic Medicine, 64(1), 71–83. doi:0033-3174/02/6401-0071
- Brown, K. W., Ryan, R. M., & Creswell, J. D. (2007). Mindfulness: Theoretical foundations and evidence for its salutary effects. Psychological Inquiry, 18(4), 211–237.
- Guardino, C. M., Dunkel Schetter, C., Bower, J. E., Lu, M. C., & Smalley, S. L. (2014). Randomised controlled pilot trial of mindfulness training for stress reduction during pregnancy. Psychology & Health, 29(3), 334-349. doi:10.1080/08870446.2013.852670
- Davis, E. (2014). Making the most of meditative moments. Toronto, ON: Barbara Gates
- Chan, K. P. (2014). Prenatal meditation influences infant behaviors.Infant Behavior and Development, 37(4), 556-561. doi:10.1016/j.infbeh.2014.06.011
- Steel, A., Adams, J., Sibbritt, D., Broom, A., Frawley, J., & Gallois, C. (2014). The influence of complementary and alternative medicine use in pregnancy on labor pain management choices: Results from a nationally representative sample of 1,835 women. The Journal of Alternative and Complementary Medicine, 20(2), 87-97. doi:10.1089/acm.2013.0171
- Jallo, N., Ruiz, R. J., Elswick, R. K., & French, E. (2014). Guided imagery for stress and symptom management in pregnant African American women. Evidence-Based Complementary and Alternative Medicine, 2014, 1-13. doi:10.1155/2014/840923
- Gedde-Dahl, M., & Fors, E. A. (2012). Impact of self-administered relaxation and guided imagery techniques during final trimester and birth. Complementary Therapies in Clinical Practice, 18(1), 60-65. doi:10.1016/j.ctcp.2011.08.008
- Lothian, J. A. (2011). Lamaze breathing: What every pregnant woman needs to know. The Journal of Perinatal Education, 20(2), 118-120. doi:10.1891/1058-1243.20.2.118
- Salvesen, K. Å., Hem, E., & Sundgot-Borgen, J. (2012). Fetal wellbeing may be compromised during strenuous exercise among pregnant elite athletes. British Journal of Sports Medicine, 46(4), 279-283. doi:10.1136/bjsm.2010.080259
- Szymanski, L. M., & Satin, A. J. (2012). Strenuous exercise during pregnancy: Is there a limit? American Journal of Obstetrics and Gynecology, 207(3), 179-187.doi:10.1016/j.ajog.2012.07.021
- Davenport, M. H., Charlesworth, S., Vanderspank, D., Sopper, M. M., & Mottola, M. F. (2008). Development and validation of exercise target heart rate zones for overweight and obese pregnant women. Applied Physiology, Nutrition, and Metabolism, 33(5), 984-989. doi:10.1139/H08-086
- Avery, N. D., Wolfe, L. A., Amara, C. E., Davies, G. A. L., & McGrath, M. J. (2001). Effects of human pregnancy on cardiac autonomic function above and below the ventilatory threshold. Journal of Applied Physiology, 90(1), 321-328.
- DeMaio, M., & Magann, E. E. (2009). Exercise and pregnancy. Journal of the American Academy of Orthopaedic Surgeons, 17(8), 504-514.
- Public Health Agency of Canada. (2012). The sensible guide to a healthy pregnancy. Ottawa, ON: Author. Retrieved form http://www.phac-aspc.gc.ca/hp-gs/guide/assets/pdf/hpguide-eng.pdf
- McGarvey, J., Thompson, J., Hanna, C., Noakes, T. D., Stewart, J., & Speedy, D. (2008). Sensitivity and specificity of clinical signs for assessment of dehydration in endurance athletes. British Journal of Sports Medicine, 44(10), 716-719. doi:10.1136/bjsm.2008.053249
- Clauson, K. A., Shields, K. M., McQueen, C. E., & Persad, N. (2008). Safety issues associated with commercially available energy drinks. Pharmacy Today, 14(5), 52-64. doi:10.1331/JAPhA.2008.07055
- Seifert, S. M., & Schaechter, J. L. (2011). Health effects of energy drinks on children, adolescents, and young adults. Pediatrics, 127(3), 511-528. doi:10.1542/peds.2009-3592
- Duong, H. T., Shahrukh Hashmi, S., Ramadhani, T., Canfield, M. A., Scheuerle, A., & Kim Waller, D. (2011). Maternal use of hot tub and major structural birth defects. Birth Defects Research Part A: Clinical and Molecular Teratology, 91(9), 836-841. doi:10.1002/bdra.20831
- Moretti, M. E., Bar-Oz, B., Fried, S., & Koren, G. (2005). Maternal hyperthermia and the risk for neural tube defects in offspring: Systematic review and meta-analysis. Epidemiology, 16(2), 216-219. doi:10.1097/01.ede.0000152903.55579.15
- Chan, J., Natekar, A., & Koren, G. (2014). Hot yoga and pregnancy: Fitness and hyperthermia. Canadian Family Physician, 60(1), 41-42.
- Pivarnik, J. M., & Mudd, L. (2009). Oh baby! Exercise during pregnancy and the postpartum period. ACSM’s Health & Fitness Journal, 13(3), 8-13. doi:10.1249/FIT.0b013e3181a1e972
- Evenson, K. R., Barakat, R., Brown, W. J., Dargent-Molina, P., Haruna, M., Mikkelsen, E. M., . . .Yeo, S. (2013). Guidelines for physical activity during pregnancy: Comparisons from around the world.American Journal of Lifestyle Medicine, 8(2), 102-121. doi:10.1177/1559827613498204
- Conger, J., & Magann, E. F. (2014). Diving and pregnancy: What do we really know? Obstetrical & Gynecological Survey, 69(9), 551-556. doi:10.1097/OGX.0000000000000105
- Hackett, D. A., & Chow, C. M. (2013). The valsalva maneuver: Its effect on intra-abdominal pressure and safety issues during resistance exercise. The Journal of Strength & Conditioning Research, 27(8), 2338-2345. doi:10.1519/JSC.0b013e31827de07d
- MacDonald, L. A., Waters, T. R., Napolitano, P. G., Goddard, D. E., Ryan, M. A., Nielsen, P., & Hudock, S. D. (2013). Clinical guidelines for occupational lifting in pregnancy: Evidence summary and provisional recommendations. American Journal of Obstetrics and Gynecology, 209(2), 80-88. doi:10.1016/j.ajog.2013.02.047
- Khatib, N., Weiner, Z., Beloosesky, R., Vitner, D., & Thaler, I. (2014). The effect of maternal supine position on umbilical and cerebral blood flow indices. European Journal of Obstetrics & Gynecology and Reproductive Biology, 175, 112-114. doi:10.1016/j.ejogrb.2013.12.043
- O’Brien, L. M., & Warland, J. (2014). Typical sleep positions in pregnant women. Early Human Development, 90(6), 315-317. doi:10.1016/j.earlhumdev.2014.03.001
- Canadian Continence Foundation. (2014). Pelvic floor exercise stimulators: To help treat incontinence (stress, urge, mixed and faecal). Retrieved from http://www.canadiancontinence.ca/pdfs/en-pelvic-floor-exercise-stimulator.pdf
- Bø, K. (2004). Pelvic floor muscle training is effective in treatment of female stress urinary incontinence, but how does it work? International Urogynecology Journal, 15(2), 76-84. doi:10.1007/s00192-004-1125-0
- Bø, K., Lilleås, F., Talseth, T., & Hedland, H. (2001). Dynamic MRI of the pelvic floor muscles in an upright sitting position. Neurourology and Urodynamics, 20(2), 167-174. doi:10.1002/1520-6777(2001)20:2<167::AID-NAU19>3.0.CO;2-4
- Ashton-Miller, J. A., & DeLancey, J. O. (2007). Functional anatomy of the female pelvic floor. Annals of the New York Academy of Sciences, 1101, 266-296. doi:10.1196/annals.1389.034
- Mørkved, S., & Bø, K. (2014). Effect of pelvic floor muscle training during pregnancy and after childbirth on prevention and treatment of urinary incontinence: A systematic review. British Journal of Sports Medicine, 48(4), 299-310. doi:10.1136/bjsports-2012-091758
- Swift, S. E. (2000). The distribution of pelvic organ support in a population of female subjects seen for routine gynecologic health care.American Journal of Obstetrics and Gynecology, 183(2), 277-285. doi:10.1067/mob.2000.107583
- Viktrup, L., & Lose, G. (2001). The risk of stress incontinence 5 years after first delivery. American Journal of Obstetrics and Gynecology, 185(1), 82-87. doi:10.1067/mob.2001.114501
- Dumoulin, C., & Hay-Smith, J. (2010). Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database of Systematic Reviews, 2010(1), 1-51. doi:10.1002/14651858.CD005654.pub2
- Hay-Smith, J., Mørkved, S., Fairbrother, K. A., & Herbison, G. P. (2008). Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women. The Cochrane Database of Systematic Reviews, 2008(4), 1-70. doi:10.1002/14651858.CD007471
- Canadian Continence Foundation. (2014). Treatment. Retrieved from http://www.canadiancontinence.ca/EN/treatment.php
- Stafne, S. N., Salvesen, K. Å., Romundstad, P. R., Torjusen, I. H., & Mørkved, S. (2012). Does regular exercise including pelvic floor muscle training prevent urinary and anal incontinence during pregnancy? A randomised controlled trial. BJOG: An International Journal of Obstetrics & Gynaecology, 119(10), 1270-1280. doi:10.1111/j.1471-0528.2012.03426.x
- Harvey, M. A. (2003). Pelvic floor exercises during and after pregnancy: A systematic review of their role in preventing pelvic floor dysfunction. Journal of Obstetrics and Gynaecology Canada, 25(6), 487-498. Retrieved from http://www.jogc.com
- Robert, M., Ross, S., Farrel, S. A., Easton, W. A., Epp, A., Girouard, L., . . . Wilkie, D. H. (2006). Conservative management of urinary incontinence. Journal of Obstetrics and Gynaecology of Canada, 28(12), 1113-1125. Retrieved from http://www.jogc.com
- Amselem, C., Puigdollers, A., Azpiroz, F., Sala, C., Videla, S., Fernández�?fraga, X., . . . Malagelada, J. (2010). Constipation: A potential cause of pelvic floor damage? Neurogastroenterology & Motility,22(2), 150-154. doi:10.1111/j.1365-2982.2009.01409.x
- Wesnes, S. L., & Lose, G. (2013). Preventing urinary incontinence during pregnancy and postpartum: A review.International Urogynecology Journal, 24(6), 889-899. doi:10.1007/s00192-013-2061
- Society of Obstetricians and Gynaecologists of Canada (SOGC) and Canadian Society for Exercise Physiology (CSEP). (2018). 2019 Canadian Guideline for Physical Activity throughout Pregnancy. Retrieved from http://csepguidelines.ca/guidelines-for-pregnancy/